Review: Early Intra Aortic Balloon Support for Heart Failure Related Cardiogenic Shock: A Randomized Clinical Trial (Alt Shock 2)
Alt-Shock2 Review
General
First Author:
Nuccia Morici, MD, PhD
Senior Author:
Federico Pappalardo, MD
Journal and Year:
JACC, 2025
Trial Registration Number (e.g., ClinicalTrials.gov):
NCT04369573
Funding Source and Conflicts of Interest:
Supported by an unrestricted grant from Getinge Global US. Several authors (e.g., Dr. Kapur, Dr. Pappalardo) disclosed relationships with various device companies; all other authors reported no relevant conflicts.
Number of sites:
7 centers (conducted in Italy)
Study Objective
Primary Aim:
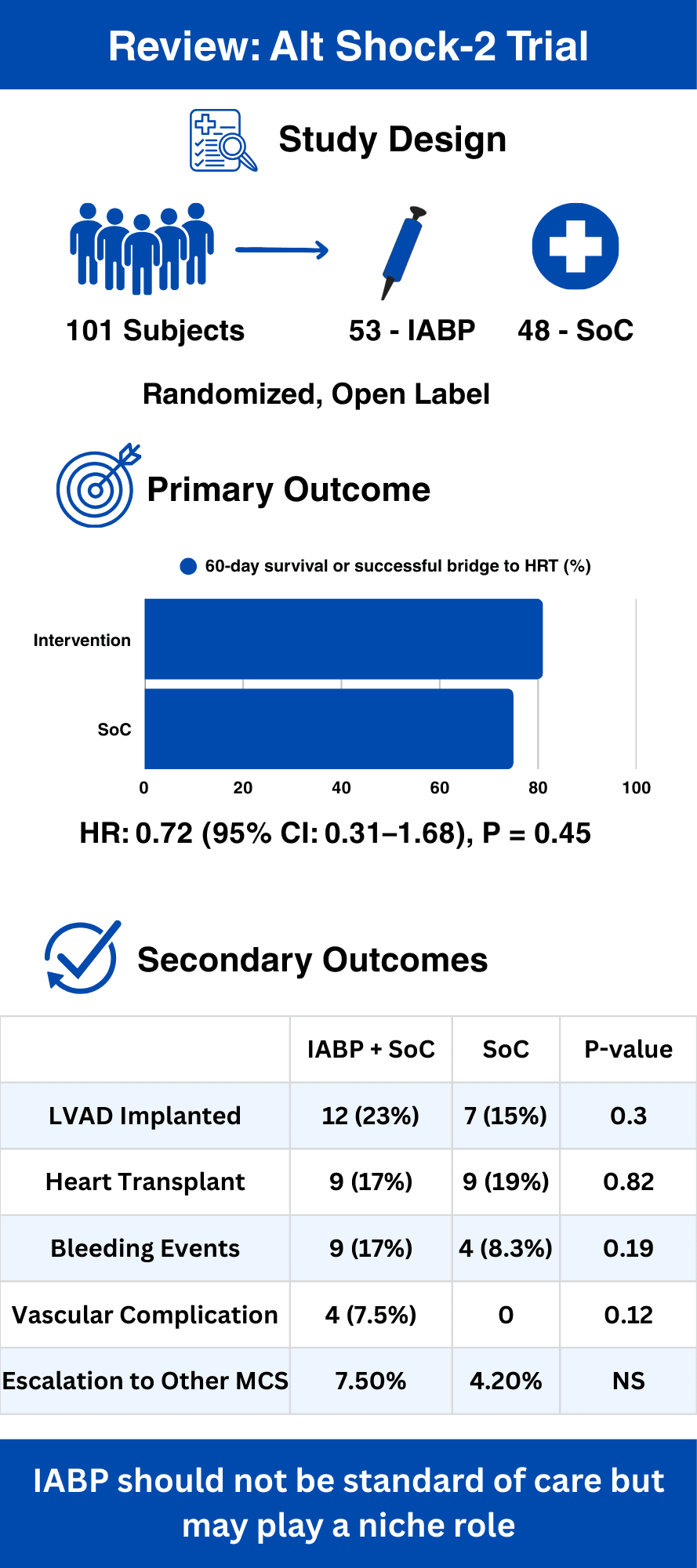
To evaluate whether early intra‑aortic balloon pump (IABP) implantation plus standard care (SoC) improves 60‑day survival or successful bridging to heart replacement therapies (HRT, including durable LVAD or heart transplant) compared with standard care alone in patients with heart failure–related cardiogenic shock (HF‑CS).
Secondary Aims (if applicable):
• To compare duration of hospitalization/CCU, maximum inotropic score, duration of inotropic therapy, and maximum sequential organ failure assessment (SOFA) score, duration of IABP support between groups.
• To assess the rates of treatment escalation (to additional temporary mechanical circulatory support devices) and adverse events (including bleeding and vascular complications).
Subgroup Analyses:
• Time between symptom onset and arrival at the coronary care unit (CCU)
• Sex
• Age
• Mean arterial pressure (MAP)
• Arterial lactate levels
• Left ventricular ejection fraction (LVEF)
• SCAI‑CSWG stage at admission
Methods
Study Design:
National, multicenter, randomized, open‑label controlled trial.
Randomized Controlled Trial (RCT), observational, crossover, etc:
RCT comparing early IABP plus standard care versus standard care alone in HF‑CS.
Blinding (single, double, open‑label, etc.):
Open‑label design; due to the nature of the intervention, treating physicians and staff were not blinded.
Study Duration (Enrollment, Follow‑up):
Enrollment occurred between June 30, 2020 and October 23, 2024. The follow‑up duration was 60 days.
Participants
Inclusion:
• LVEF <= 35%, SCAI B-D shock according to the CSWG Definition (JACC 2022)
• Age 18 to 75 years
• Need of vasoactive agent to maintain SBP > 90 mmHG or, MAP > 60 mmHg
Exclusion:
• Septic shock with an evident focus
• Severe peripheral vascular disease
• Cardiogenic shock secondary to cardiac or noncardiac surgery
• Acute myocardial infarction within 1 month or suspected/documented myocarditis
• Pulmonary embolism
• Chronic end‑stage organ dysfunction precluding HRT or life expectancy <1 year
• Pregnancy or lactation
• Any other significant condition that could put the patient at risk or affect participation
Intervention(s)
IABP + SoC Group:
Early IABP implantation immediately after randomization, performed either at the bedside or in the catheterization laboratory per institutional protocols.
The device (from either Arrow or Getinge) was selected based on patient characteristics, with prophylactic anticoagulation administered.
Standard care included vasoactive and inotropic support per local practice.
Standard Care (SoC) Group:
Received standard care based on local practices with vasoactive agents and inotropes, without early IABP implantation.
Statistical Analysis
• The primary endpoint (60‑day survival or successful bridge to HRT) was analyzed in the intention‑to‑treat (ITT) population using Kaplan‑Meier estimates and an unadjusted Cox proportional-hazards model.
• Continuous variables were summarized as medians (with interquartile ranges) and categorical variables as frequencies and percentages.
• Comparisons were made using chi‑square or Fisher’s exact tests for categorical variables and Student’s t-test for continuous variables.
• A per‑protocol (PP) analysis was also performed as supportive evidence.
• The trial was originally designed for 200 subjects (100 per group) with a group sequential design, but an interim analysis led to early trial termination for futility.
Results
Participants:
• Out of 787 patients screened, 101 patients were enrolled and randomized – 53 to the IABP + SoC group and 48 to the standard care group.
• The final ITT analysis included all 101 patients.
Baseline Characteristics:
• Median age: 60 years (IQR: 54–65)
• 80% were male
• Median systolic blood pressure ~90 mm Hg
• Median left ventricular ejection fraction: 20% (IQR: 15–24%)
• Approximately 54–68% of patients had nonischemic cardiomyopathy
• Other variables (e.g., arterial lactate levels, body mass index) were similar between groups
• (Detailed baseline characteristics are provided in Table 1.)
Primary Outcome:
The composite endpoint of 60‑day survival or successful bridge to HRT was achieved in 43 patients (81%) in the IABP + SoC group versus 36 patients (75%) in the standard care group.
• Hazard ratio (HR): 0.72; 95% confidence interval (CI): 0.31–1.68; P = 0.45.
Secondary Outcomes:
• No significant differences were found between groups in terms of:
• Maximum inotropic score
• Maximum SOFA score
• Duration of inotropic therapy
• Duration of hospitalization (overall and CCU)
• Rates of treatment escalation (e.g., escalation to additional MCS such as Impella or ECMO)
• Adverse events including bleeding, vascular complications, and other listed events
• Bridging to HRT (heart transplant or durable LVAD) was achieved in 33% of standard care patients versus 39.6% in the IABP group (P = 0.52).
(See Tables 2 and 3, and Figure 2 for Kaplan‑Meier curves.)
Subgroup Analysis:
• Subgroup analyses (presented in Figure 3) did not show statistically significant interactions between treatment effect and variables such as time from symptom onset to CCU, sex, age, MAP, arterial lactate, LVEF, or SCAI‑CSWG stage.
Strengths and Limitations
Strengths:
• Prospective, randomized design focused specifically on a well‑defined HF‑CS population using updated SCAI criteria.
• Multicenter trial with rigorous data collection and centralized randomization.
• Comprehensive assessment of both efficacy (60‑day survival or bridge to HRT) and safety endpoints.
• Detailed subgroup and per‑protocol analyses provided supportive data.
Limitations:
• Open‑label design may introduce performance bias, although endpoints were objectively measured.
• Early termination for futility resulted in a smaller sample size than originally planned, potentially underpowering the study.
• Slow recruitment and a highly selected patient population may limit generalizability.
• Heterogeneity in underlying etiologies of HF‑CS and variable access to HRT across centers.
• Lack of standardization in IABP management protocols (e.g., anticoagulation, device optimization).
Implications for Clinical Practice
The Alt‑Shock 2 trial indicates that routine early IABP implantation in patients with heart failure–related cardiogenic shock does not significantly improve 60‑day survival or successful bridging to heart replacement therapies compared with standard care alone. These findings suggest that the routine use of IABP in this specific HF‑CS population is not supported.